Bone Degradation Measure Can Sway Osteoporosis Diagnosis
Assessing a key aspect of bone architecture, for which clinicians can now be reimbursed under Medicare, can significantly improve the ability to predict a patient’s risk for bone fracture.
Although bone mineral density (BMD) is traditionally used to identify patients with osteoporosis or low bone mass, some physicians have begun incorporating the trabecular bone score (TBS) into their exams.
At the Cleveland Clinic Center for Specialized Women’s Health in Ohio, factoring in the TBS changed the diagnosis for 16% of 432 patients, according to Holly Thacker, MD, the center’s director.
“Importantly, 11% got worse diagnoses, and I use that in terms of prioritizing treatment,” Thacker told Medscape Medical News. The ability to determine how degraded the bone microarchitecture is through a software system “is a huge advance.”
Thacker described her center’s experience with the technology at the 2023 Menopause Meeting in Philadelphia.
While BMD captures the amount of minerals like calcium in the skeleton, TBS assesses the underlying microarchitecture by looking at the distribution of shades of gray on dual-energy x-ray absorptiometry (DEXA) scans.
Based on the TBS, patients’ bones are classified as normal, partially degraded, or degraded. Among the 432 patients who received a TBS analysis in 2022, 3% shifted from a normal diagnosis to osteopenia, or subclinically low bone density; 8% worsened from osteopenia to osteoporosis; 4% went from osteopenia to normal; and 1.6% downgraded from osteoporosis to osteopenia, Thacker reported.
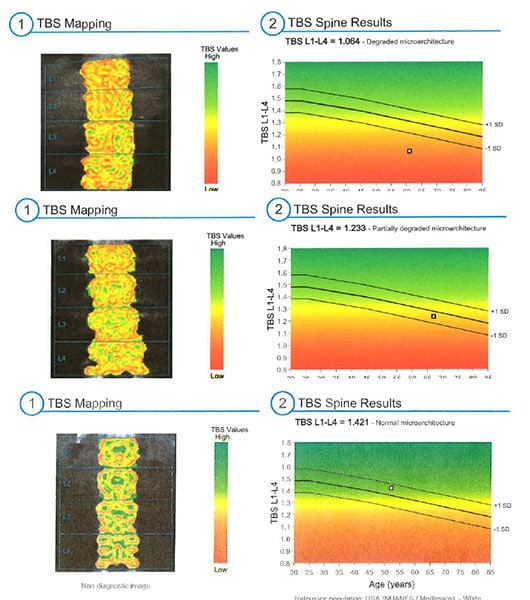
(From top to bottom): TBS results for a 61-year-old patient with degraded bone, a 67-year-old patient with partially degraded bone, and a 52-year-old patient with normal bone.
The new test may also provide some reassurance for female patients who have thinner bones, which may raise alarms based on BMD. TBS, however, may show that the structure of the bone looks normal.
“When you know that the microarchitecture is normal, you’re a lot less concerned that they actually have a bone disease of osteoporosis,” Thacker said.
Conversely, unexpectedly degraded bone raises questions.
“That makes you go back and say [to the patient], ‘Have you been on steroids? Were you malnourished? Is there some other metabolic problem? Have you had some calcium disorder?’ ” Thacker said.
Thacker leverages the TBS to help patients obtain effective therapy, typically an anabolic agent followed by antiresorptive medication, she said.
“When I see a patient who not only has osteoporosis on bone density but has completely degraded bone architecture, it’s a lot easier for me to make the argument to the insurance company that this patient is at grave risk for a low trauma fracture and bad outcome without the best treatment,” Thacker said.
10-Year-Old Tech, Recently Covered
The US Food and Drug Administration approved TBS software in 2012, but Medicare only recently started paying for it.
Medimaps Group, a company that markets imaging software to calculate TBS, announced in 2022 that reimbursement from the Centers for Medicare & Medicaid Services (CMS) was available, at $41.53 on the Physician Fee Schedule and $82.61 on the Hospital Outpatient Prospective Payment Schedule.
“Reimbursement through CMS is an important endorsement of the clinical value of TBS for clinicians and their patients,” said Didier Hans, PhD, MBA, the CEO of Medimaps, in a statement at the time. He noted that more than 600,000 TBS procedures were being performed in the United States each year.
“TBS is going to be most helpful in those with osteopenia who are right near the threshold for treatment,” said Dr Marcella Donovan Walker of Columbia University in New York City.
Nevertheless, the initial investment in purchasing the software may be a barrier for health systems.
“We are the first and only site in our health system to offer TBS, as this is an extra expense and not uniformly reimbursed by insurers,” Thacker reported at the meeting.
Potential Drawbacks
The TBS software used in Thacker’s study has been validated only in Asian and White patients between certain ages and weights, meaning the system is not designed to be used for other populations. Other researchers have highlighted a need for trabecular bone scoring to be validated more broadly. The authors of a recent analysis, however, suggest that TBS can be used the same way no matter a patient’s race.
TBS “is going to be most helpful in those with osteopenia who are right near the threshold for treatment,” said Marcella Donovan Walker, MD, MS, in a presentation on bone quality at the Menopause Meeting.
Many studies have shown that TBS “provides additive information to bone density,” said Walker, a professor of medicine in the division of endocrinology at Columbia University College of Physicians and Surgeons in New York City. For example, a large study of women in Manitoba, Canada, found that regardless of whether their bone density was normal, osteopenic, or osteoporotic, those with a low TBS had a much higher risk for fracture, Walker said.
“Opportunistic Screening” With CT?
TBS relies on the same DEXA scans that are used to calculate bone mineral density, so obtaining the score does not add time or radiation to the scanning process, Thacker said.
But many patients who should receive DEXA scans do not, which adds to the promise of “opportunistic screening” for osteoporosis, Walker said. With this approach, physicians would analyze a CT scan that a patient received for another purpose, such as to investigate abdominal pain or chest pain.
“In these images is information about the bone,” Walker said.
Researchers have used high-resolution peripheral quantitative CT to perform finite element analysis, where a computer program simulates compression of the bone to create a measure of bone stiffness and determine the load required for a break.
One study found that including those elements predicted fractures better than bone mineral density or the Fracture Risk Assessment Tool (FRAX) alone, Walker noted.
Other aspects of bone quality include how many cracks are in the bone, the amount of adipose in the marrow space, and the rate at which bone is broken down and rebuilt. But Walker suggested that the longstanding focus on bone mineral density in clinical practice makes sense.
“By far, bone mass is the most important bone quality,” Walker said.
Thacker is the executive director of the nonprofit Speaking of Women’s Health. Walker disclosed funding from the National Institute of Arthritis and Musculoskeletal and Skin Diseases and Amgen.
For more news, follow Medscape on Facebook, X (formerly Twitter), Instagram, YouTube, and LinkedIn
Source: Read Full Article