problems with topamax

Hysterosalpingography (often abbreviated as HSG) is a diagnostic imaging technique used primarily in the investigation of female infertility. It has been in use for a hundred years, with the first one having been performed in 1917.
Many uterine problems may be diagnosed with the help of this test, including congenital anomalies of the uterus and tubes, but also any polyps, submucous fibroids, synechiae (adhesions between the walls of the uterus or tubes), and adenomyosis (growth of the endometrial lining deep into the underlying myometrium or muscular layer).
Abnormalities of the tubes that may be picked up by HSG include tubal blockage, salpingitis isthmica nodosum (an inflammatory scarring condition of the tubes), polyps, hydrosalpinx (accumulation of serous fluid in a dilated portion of one tube), and adhesions between the tube and surrounding structures which hinder its normal motility and the passage of gametes through it.
Purpose
The primary purpose for pursuing an HSG is to find out if the fallopian tubes, leading between the upper corners of the uterus and the ovaries, are patent and if their form is normal. The tubes normally appear as smooth thin outlines of contrast medium on the proximal side, dilating in the ampullary portion on the distal side, near the ovaries.
The type of abnormalities that may be present in the tubes may be classified as congenital or acquired blockages due to spasm of the tubes. True blockage may be seen if present as the absence of contrast beyond that point. Infection can also be picked up, as may be peritubal adhesions which kink the tube or keep the contrast material bottled up, mimicking its spread at the fimbrial end or a hydrosalpinx. Any of these changes may be bilateral or unilateral.
This technique is quite sensitive at detecting abnormalities of the uterine cavity, but its specificity is low, so that hysteroscopy is generally preferred for this purpose.
Technique
An HSG involves the injection of contrast material into the cervix using a slender microcatheter. Either oil-soluble or water-soluble contrast media are used. The timing is important, as it is usually performed 2 or 3 days after the cessation of the menstrual bleed.
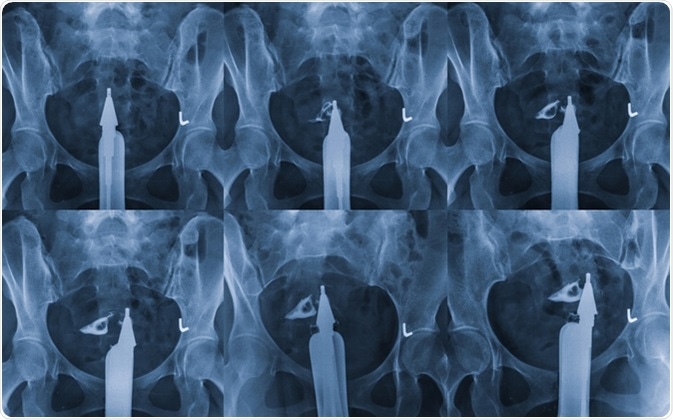
The contrast passes upward (in a retrograde manner) into the uterine cavity, the fallopian tubes, and any other openings that are patent. An X-ray is taken, and its findings determine whether the tube is patent. It thus provides a radio-opaque outline of these hollow organs, and helps to determine whether the tubes are abnormally dilated, blocked or patent, by visualizing how the dye passes along them and eventually pools near the fimbrial end. The cannula used to perform dye injection should be as small as it can be to introduce the dye without backflow from the cervix.
An HSG positive for tubal abnormality should be confirmed by repeating it. The causes may include endometrial polyps, a fibroid, or an anatomical variation in the structure of the uterus and/or tubes. Repeat X-rays are taken of the dye-filled uterus and tubes at various stages.
Type of Contrast and Fluoroscopy
Either a water-soluble or oil-based contrast agent is used. The oil-based medium is preferable to break down slight adhesions and has been linked to better pregnancy rates following the procedure without any additional treatment. This is associated with granuloma formation within the tubes due to irritation, especially if the tubes are already infected or inflamed. For this reason, water-soluble contrast is used in most centers nowadays.
This practice may change, however, with the very recent finding that 40% of women conceived within 6 months after having a HSG using ethiodized oil (i.e. an oil-based iodine-containing agent), while 30% of women did with a water-based agent being used.
The whole process is done under fluoroscopy, a type of low-intensity continuous X-ray screening with image intensification technology, to yield repeated images as the dye is injected and makes its way through the reproductive organs.
The pressure and speed at which the dye is injected should be carefully monitored. If it is injected too fast, or too much of it is inserted, it may extravasate into the vessels or hide the area around the fimbrial ends of the tubes. Too little injection at too low a pressure may fail to show the contour of the uterine cavity, tubes and fimbriae clearly, making it of low utility.
Precautions
Any woman who has an HSG should be instructed to come in 2-3 days after her period ends (in the follicular phase of the menstrual cycle), and a pregnancy test should be performed, so that pregnancy is excluded. If the patient is pregnant the fetus may be exposed to radiation.
Since the cause of infertility may be shared by both partners, the European Society of Human Reproduction and Embryology (ESHRE) advises that both a semen analysis and ovulation testing should be done first before an HSG is recommended.
Advantages
- An HSG is a non-invasive procedure, apart from the cannulation of the cervix to introduce the dye
- It is inexpensive compared to laparoscopy and other diagnostic tests
- It can identify some uncommon conditions such as uterine fistulas by the spilling of dye through the abnormal opening
- The procedure is followed by spontaneous conception in a percentage of couples who had earlier been unable to conceive (probably by the breaking up of slight adhesions or the clearing away of debris by the passage of the contrast medium) which is higher with oil-soluble contrast – thus, it can be both diagnostic and therapeutic in some cases
Complications
- An HSG may cause cramping pain in the lower abdomen as the cannula is passed through, and dye is injected into the uterine cavity. While usually slight and resolving quickly, in a few cases it may become severe or patient may faint due to the stimulation of the vagal nerve, which called a vasovagal reaction. It may lead to the procedure being stopped before the necessary data is gathered.
- Uterine bleeding and infection may occur, thus prophylactic antibiotics are administered if appropriate
- The uterus may be accidentally perforated by the passage of the cannula
- The patient may suffer a hypersensitivity reaction to the contrast agent used, which may even include anaphylaxis
Sources
- www.umm.edu/health/medical/reports/articles/infertility-in-women
- cursoenarm.net/…/36478?source=see_link
- www.mayoclinic.org/…/drc-20354313
- https://www.ncbi.nlm.nih.gov/pubmed/15950625
- https://www.ncbi.nlm.nih.gov/pubmed/16549607
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3443271/
- https://www.ncbi.nlm.nih.gov/pubmed/3826199
- www.omicsonline.org/…/…lity-a-review-article-2167-0420.1000176.php
- https://academic.oup.com/humrep/article/26/5/967/674503
- https://www.adelaide.edu.au/news/news92362.html
Further Reading
- All Hysterosalpingography Content
- Complications of Hysterosalpingography
- Indications and Contraindications for Hysterosalpingography
- Technique and Precautions During Hysterosalpingography
Last Updated: Feb 26, 2019

Written by
Dr. Liji Thomas
Dr. Liji Thomas is an OB-GYN, who graduated from the Government Medical College, University of Calicut, Kerala, in 2001. Liji practiced as a full-time consultant in obstetrics/gynecology in a private hospital for a few years following her graduation. She has counseled hundreds of patients facing issues from pregnancy-related problems and infertility, and has been in charge of over 2,000 deliveries, striving always to achieve a normal delivery rather than operative.
Source: Read Full Article