nexium 10
Where to buy cheap zoloft from india no prescription
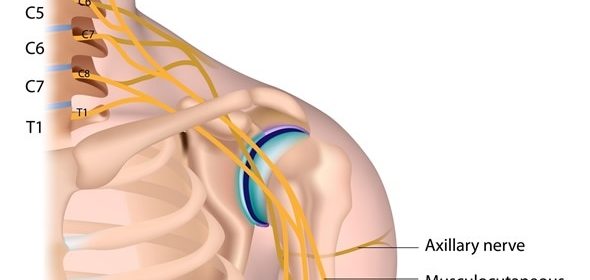
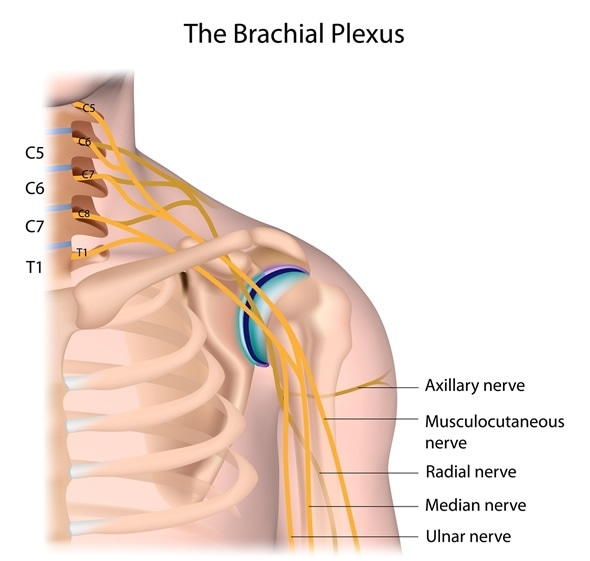
Erb-Duchenne and Dejerine-Klumpke are palsies of the brachial plexus. Palsy refers to paralysis while brachial plexus is the network of nerves in the region from the neck down towards the shoulder, arm, and hands. Erb-Duchenne palsy refers to the paralysis of the upper brachial plexus. It affects the upper arm. Dejerine-Klumpke palsy refers to the paralysis of the lower brachial plexus. It affects the lower arm and hand.
Neonatal Birth Defects
Erb-Duchenne and Dejerine-Klumpke are injuries of the brachial plexus which may occur at any time, but they have been known to occur in neonatal cases with difficult deliveries. The palsy may be caused because the infant’s head and neck are pulled to a side as the shoulders come through the birth canal. The shoulder of the infant may have been stretched during a normal delivery to cause the injury.
Injury may also be caused by pressure on the infant’s raised arms in a breech delivery where the infant comes out feet first from the birth canal. There may be possibility of neonatal brachial plexus injuries if the infant is larger in size than average and has difficulty is passing through the birth canal.
Chance of the neonatal birth injury causing permanent damage is 3 to 25% depending on the severity of the damage to the nerve. Both genders are equally likely to be affected during difficult births. The palsy condition is usually identified soon after birth when the attending health care practitioner checks for motor responses.
Types of Brachial Plexus Injuries Leading to Erb-Duchenne and Dejerine-Klumpke
The network of five nerves located in the brachial plexus can suffer four primary types of injuries leading to paralysis of the upper or lower part of the arm. These are:
1. Avulsion: This is the most severe type of injury to the brachial plexus wherein the nerve is torn from the spine completely. This injury has the scope of partial recovery post surgery.
2. Rupture: In this injury, the nerve located in the brachial plexus is torn, but it is still attached to the spinal chord. Surgery will be required.
3. Neuroma: Here the nerve has been damaged but managed to heal, however the scar tissue makes the nerve unable to conduct electrical impulses through the muscles. Surgery may not be required.
4. Neuropraxia: While the nerve is damaged, it is not torn. This is the most common type of brachial plexus injury. Spontaneous recovery of nerve takes place over time.
Any of these injuries to the brachial plexus will lead to a paralysis of the affected arm. This could manifest in severity from complete lack of control of the muscles to a lack of sensation in the arm.
How are Erb-Duchenne and Dejerine-Klumpke Diagnosed?
The neonatal birth injury is suspected when no movement is made by the upper or lower arm of the infant. The arm may lie limply at the side of the infant or it is bent at the elbow and held against the side. If the injury is not very severe it may be just the grip of the infant that is weakened.
In the physical examination, the arm may flop uncontrolled when the infant is rolled from side to side. There may be no reflex on the side where the brachial plexus palsy exists. An X-ray may be required to rule out fracture of the collarbone causing pseudoparalysis.
For older patients who can comment on the loss of control or lack of sensation in the arm, other tests like electromyography, magnetic resonance imaging, and computerised tomography may be suggested by the attending physician in order to confirm nerve damage of the brachial plexus. The patients may be able to help with the diagnosis of traumatic brachial plexus palsy by providing information about how the injury was sustained.
Treatment and Prognosis for Erb-Duchenne and Dejerine-Klumpke
In neonatal brachial plexus palsies which are not too severe, the infant’s prognosis is quite good. With regular massages and some physiotherapy, the infant will regain full control of the arm within three to nine months time.
In case there has been no improvement by the time the infant is nine months old, surgery will be recommended. This could take the form of nerve grafts and nerve transfer, wherein healthy nerves are harvested from other parts of the body to replace the damaged nerves in the brachial plexus.
For older patients, there is no option but surgery in case of avulsion and rupture injuries. These are usually caused by external traumas such as being involved in motor accidents or sports injuries. For neuroma and neuropraxia injuries, the prognosis will differ based on the extent of nerve damage. These injuries do not require surgical intervention and make a spontaneous recovery with 90 to 100% return of function in the arm.
References
- http://www.birthinjuryguide.org/birth-injury/types/klumpkes-palsy/
- http://www.ninds.nih.gov/disorders/brachial_plexus_birth/brachial_plexus_birth.htm
- https://medlineplus.gov/ency/article/001395.htm
- http://emedicine.medscape.com/article/317057-overview
Further Reading
- All Brachial Plexus Content
- Brachial Plexus
Last Updated: Feb 26, 2019

Written by
Cashmere Lashkari
Cashmere graduated from Nowrosjee Wadia College, Pune with distinction in English Honours with Psychology. She went on to gain two post graduations in Public Relations and Human Resource Training and Development. She has worked as a content writer for nearly two decades. Occasionally she conducts workshops for students and adults on persona enhancement, stress management, and law of attraction.
Source: Read Full Article