coumadin therapy nutrition
Cheap crestor ca without prescription
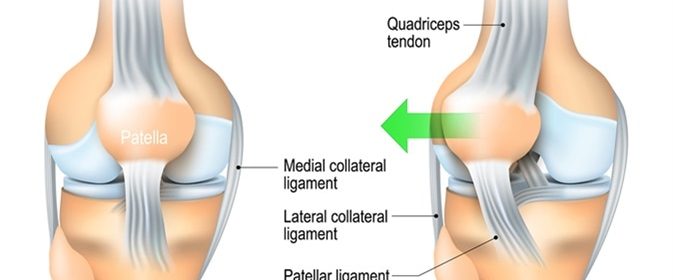
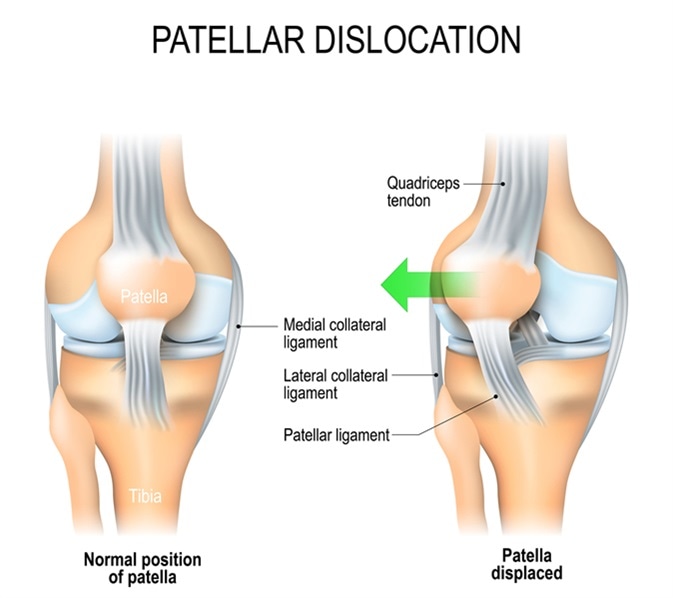
The kneecap or patella is a triangular piece of bone that protects the front of the knee joint. It may get dislocated when the leg suddenly changes direction and the foot is planted on the ground, putting great stress on the kneecap.
In most cases, the dislocation is towards the outside of the knee. It affects about 6 per 100,000 of the population, being most common in active adolescence (29 per 100,000).
Causes
The kneecap may become unstable and thus becomes liable to dislocation owing to factors, such as:
- Abrupt swinging or rotation of the body with a solidly planted foot
- Direct impact on the patella with a solid object
In children, it may also occur in the following circumstances:
Abnormality of the Knee Joint
- If the articular surface of the femur is very shallow, dislocation is more prone to occur even with a minimal force
- Laxity of the knee ligaments is another predisposing factor and is seen especially in girls
- The patellar tendon is inserted abnormally on the tibia
- Genu valgum or knock knees with an altered line of tracking of knee flexion-extension
- High knee cap
- Cerebral palsy and Downs syndrome are conditions in which the kneecaps are prone to dislocation because of muscle weakness and imbalance between opposing groups of muscles
- Patellar instability of congenital origin, often painless
- A shallow and irregular groove in the femur which makes the patella more susceptible to dislocate
Normal Knee Joint
On the other hand, children with anatomically normal knee joints may suffer kneecap dislocation because of falling on the knee or hitting the knee against something hard commonly observed in high-impact sports injuries.
A third group is a non-contact dislocation, as when the body is swung forcefully with a firmly planted foot, commonly experienced by a baseball player, when torso rotates and the right foot is planted on the ground.
Symptoms
A patellar dislocation may present with:
- A misshapen or deformed knee
- Inability to straighten a knee which is fixed in the flexed position
- Feeling the kneecap shift on the outside of the groove
- Feeling the patella dislocation, with a popping sound
- Knee pain
- Swelling of the knee which is tender on touch
- “Sloppy” or hypermobile kneecap, which can be shifted too freely from one side to the other
- The “apprehension” sign which refers to the patient’s anxiety during running or when the doctor moves the patella laterally to reproduce the dislocation
With the first or second episode of patellar dislocation, pain is usually present, and the individual cannot walk. The child may also unconsciously fear to change the direction while running.
Repeated untreated episodes lead to less pain with each dislocation, as the ligaments become lax. This does not change the fact that the joint cartilage is being damaged by the subluxated patella.
Diagnosis and Treatment
The symptoms followed by a physical examination will usually be sufficient to make the diagnosis. A knee X-ray and MRI if required will exclude any fracture or articular trauma, bone bruising during reduction of the dislocation, and tears of the anterior cruciate ligament in the knee joint. These tears should always be excluded as they occur in the same type of situations and are more commonly seen than patellar dislocations.
Once the diagnosis is clear, the dislocation is reduced. Knee immobilization will keep the patella in position until the ligaments heal, usually for about 3 weeks. During this time, weight bearing is not advised.
Physical therapy is important after the cast is removed, to build up muscle strength and range of motion at the joint. The patient is typically able to resume normal activity in about 3-6 weeks, depending on age, health, and severity of the injury.
Arthroscopic or sometimes open repair may be done if the bone or cartilage is damaged or there is persistent instability at the kneecap. Congenital abnormalities of the bones should also be corrected to prevent recurrences.
Prognosis
Recurrent patellar dislocation may be due to lack of timely and adequate treatment or due to the presence of anatomical knee joint aberrations. Cycling and other exercises may be of great use in strengthening the muscles around the joint and thus stabilizing the patella. The risk of repeated dislocation is about 20% to 40% and after a second dislocation, the risk is about 50%. This is even higher in patients below the age of 25 years because the epiphysis is damaged affecting growth, and up to 70% of these individuals have repeated dislocations. Such patients should, therefore, undergo a stabilizing surgery if they are active in sports or demanding physical occupations.
Sources
- https://medlineplus.gov/ency/article/001070.htm
- orthoinfo.aaos.org/…/
- www.patellofemoral.org/…/…nt_of_Pediatric_Patellar_Dislocation.pdf
- www.hss.edu/conditions_patellofemoral-disorders-overview.asp
- https://patient.info/doctor/knee-fractures-and-dislocations
- www.cedars-sinai.edu/…/Kneecap-Patellar-Dislocation.aspx
Further Reading
- All Kneecap Content
Last Updated: Feb 26, 2019

Written by
Dr. Liji Thomas
Dr. Liji Thomas is an OB-GYN, who graduated from the Government Medical College, University of Calicut, Kerala, in 2001. Liji practiced as a full-time consultant in obstetrics/gynecology in a private hospital for a few years following her graduation. She has counseled hundreds of patients facing issues from pregnancy-related problems and infertility, and has been in charge of over 2,000 deliveries, striving always to achieve a normal delivery rather than operative.
Source: Read Full Article