buy generic coreg coupons no prescription
https://greenhealthlive.com/top/generic-aricept-australia-no-prescription/
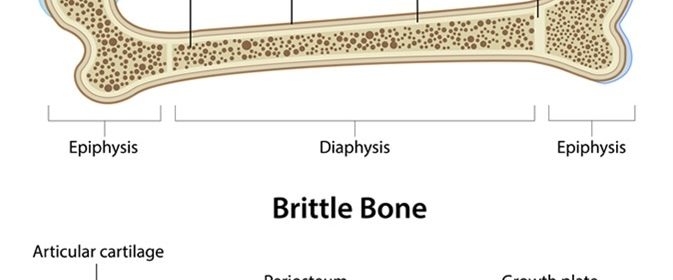
Brittle bone disease or Osteogenesis Imperfecta (OI) is characterized by a fragile skeleton. The mutation in the genes, COL1A1, COL1A2, CRTAP, and P3h2 result in OI. In most cases, the inheritance pattern is autosomal dominant and in some cases it could also be autosomal recessive. The gene mutation affects the formation and strength of the bone while affecting other body systems. Broken bones are very common and increase in the later life of the patients. A life-long disorder, it occurs across races irrespective of sex.
.jpg)
Types of OI
There are eight major types classified into mild, moderate, or severe OI:
- Mild: Type 1
- Moderate: Type 4, 5, 6 and 7
- Severe or most severe: Type 2, 3, and 8
Mild forms of OI
Type I, the most common and mild form of OI, characterized by mild fragile bone, few fractures, and minimal malfunction of the limb, is dominantly inherited. When a child starts to walk, the bone might have a fracture or experience dislocations of the shoulder and the elbow. In some children, long bones are prone to multiple fractures, vertebrae may experience compression fractures, and chronic pain is evident. However, the time period between the fractures may vary significantly. Even though the stature of the child with OI may be slightly short compared with non-OI children, the stature will be within the normal age ranges. Occurrence of hearing loss will be high beginning from early childhood. Type 1 collagen will be lower, while the structure of the collagen will be normal.
Moderate forms of OI
Retarded growth is a significant factor that distinguishes OI Type IV from OI Type I. Severity of the retardation may vary from moderate to severe. The Child will be shorter or of less than average height for their age, with short humerus and femur. The child will have a fracture when learning to walk. Scoliosis, compression of the vertebrae, fractures in long bone, ligament laxity, and bowed long bones are common. The inheritance pattern in OI Type IV is autosomal dominant and does not involve type 1 collagen deficiency; however, it is reduced in bone matrix. The color of the sclera is light blue in infants with varied intensities of the color. The color may turn to white later, or in young adults.
Inherited dominantly, the fracture frequency and the degree of skeletal malformation in OI Type V are comparable to OI Type IV.
OI Type VI is very rare and is characterized by distinctive mineralization defect in bone biopsy.
Short stature, Coxa vara, and shorter leg bones, humerus, and femur are common in Type VII OI. The appearance and symptoms of some cases of OI Type VII are analogous to OI Types IV in many aspects. The recessive inheritance of CRTAP gene mutation causes OI Type VII, which is considered to be a moderate form of OI.
Severe forms of OI
Type II, the most severe form of OI, is characterized by low weight, soft skulls, small chests, and very small limbs in infants. Legs will be in frog-leg position and in the vertebrae, long bones and skull, intrauterine fractures will be obvious. Most of the infants die within a few weeks of birth due to complications arising in the respiratory and cardiac system. While a few infants may live longer, the lungs are underdeveloped and respiratory and swallowing problems are common. Type 1 collagen gene mutation or parental mosaicism is the cause of OI Type 2.
Characterized by dominant gene mutations in collagen type 1 that are spontaneous, children who stay alive in the neonatal period are prone to OI Type III.
At birth, symptoms are slightly short and bowed limbs, soft calvarium, and smaller chests. Infants face problems with respiration and swallowing. Due to growth plates disruption the deformity is progressive. Children will have short stature and in adulthood the height of the individual will be less than 3 feet.
As type I collagen is reduced in the bone matrix, many long-bone fractures can occur while the degree of fragility of the bone and the rate of fracture rate may vary significantly. Frequently, the individuals suffer from spine curvatures, scoliosis, chest abnormalities, long bone fractures, and vertebrae will experience compression fractures.
A large head, under-developed face bones, and the triangular face shape are characteristic of OI Type III. The color of the sclerae will be gray, white, purple or tinted blue. Though Dentinogenesis imperfecta is not widespread, it is common in OI Type III. The LEPRE1 gene mutations may lead to absence or severe deficiency of prolyl 3-hydroxylase activity resulting in OI Type VIII. Severe deficiency in growth and under-mineralization of the skeleton will be extreme in these types. The appearance and symptoms are analogous to OI Types II or III in terms of appearance and symptoms with white sclerae being the only exception.
Sources
- http://www.oif.org/site/PageServer?pagename=AOI_Facts
- www.netdoctor.co.uk/…/
- www.niams.nih.gov/…/osteogenesis_imperfecta_ff.asp
- https://ghr.nlm.nih.gov/condition/osteogenesis-imperfecta
Further Reading
- All Osteogenesis Imperfecta Content
- Osteogenesis imperfecta (OI)
Last Updated: Aug 23, 2018

Written by
Afsaneh Khetrapal
Afsaneh graduated from Warwick University with a First class honours degree in Biomedical science. During her time here her love for neuroscience and scientific journalism only grew and have now steered her into a career with the journal, Scientific Reports under Springer Nature. Of course, she isn’t always immersed in all things science and literary; her free time involves a lot of oil painting and beach-side walks too.
Source: Read Full Article