Web tool aims to better inform and refine need for treatment in early prostate cancer

A new tool to predict an individual’s prognosis following a prostate cancer diagnosis could help prevent unnecessary treatment and related side effects, say researchers at the University of Cambridge.
The tool, PREDICT Prostate, launches today to coincide with publication in the journal PLOS Medicine of the research that underpins it. It brings together the latest evidence and mathematical models to give a personalised prognosis, which the researchers say will empower patients as they discuss treatment options with their consultant.
According to Cancer Research UK, there were 47,151 new cases of prostate cancer in 2015. Progession of the disease, which usually presents in later life, is very variable: in most cases, the disease progresses slowly and is not fatal. It is often said that more men die with prostate cancer than from it. However, it is still the case that in a significant number of men, the tumour will metastasise and spread to other organs, threatening their health.
When a patient is diagnosed with prostate cancer, they are currently classified as low, intermediate or high risk. Depending on the patient’s risk group, clinicians will recommend either an ‘active monitoring’ approach or treatment. Treatment options include radiotherapy or surgery and can have potentially significant side-effects, including erectile dysfunction and urinary incontinence.
However, evidence suggests that these classifications, which are in the current guidelines provided by the National Institute for Health and Care Excellence (NICE), are only 60-70% accurate. This means that many men may elect for treatment when it is not necessary. In fact, a recent study carried out in the UK showed that for early prostate cancer (low and intermediate risk), treatment is no more beneficial in terms of ten year survival compared to no treatment.
Cambridge researchers have already shown that it is possible to improve the accuracy of the NICE-endorsed model to more than 80% by stratifying patients into five rather than three groups. Their next challenge was to use this information to give a more individual prediction of outcome to patients at no extra cost. The result is PREDICT Prostate.
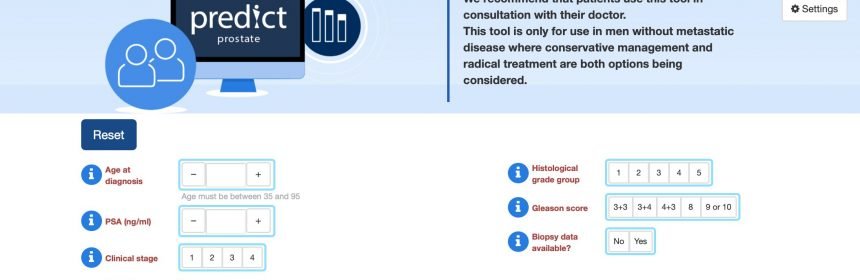
PREDICT Prostate takes routinely available information including PSA test results, the cancer grade and stage, the proportion of biopsies with cancerous cells, and details about the patient including his age and other illnesses. It then gives a 10-15 year survival estimate. Importantly, the tool also estimates how his chance of survival differs depending on whether he opts for monitoring or treatment, providing context of the likelihood of success of treatment and risk of side effects.
“As far as we are aware, this is the first personalised tool to give an overall survival estimate for men following a prostate cancer diagnosis,” says first author Dr. David Thurtle, Academic Clinical Fellow in Urology at the University of Cambridge and Addenbrooke’s Hospital, which is part of Cambridge University Hospital NHS Foundation Trust (CUH).
“PREDICT Prostate is designed for men who are considering whether to choose to monitor or to opt for treatment. This is the choice that faces nearly half of all men who are diagnosed with prostate cancer. We hope it will provide a more accurate and objective estimate to help men reach an informed decision in discussion with their consultant.”
The research was led by Dr. Vincent Gnanapragasam, University Lecturer and Honorary Consultant at CUH, and undertaken by Dr. Thurtle, both of the Academic Urology Group in Cambridge, and in collaboration with Professor Paul Pharoah of the Department of Cancer Epidemiology.
“We believe this tool could significantly reduce the number of unnecessary—and potentially harmful—treatments that patients receive and save the NHS millions every year,” says Dr. Gnanapragasam.
“This isn’t about rationing treatments—it’s about empowering patients and their clinicians to make decisions based on better evidence. In some cases, treatment will be the right option, but in many others, patients will want to weigh up the treatment benefits versus the risks of side effects. It will also show men who do need treatment a realistic estimate of their survival after treatment.”
Data from the National Prostate Cancer Audit has shown that rates of treatment for low risk prostate cancer vary across different hospitals between 2-25%. ‘Radical’ treatment—surgery or radiotherapy, for example—costs on average around £7,000 per patient and treating these men unnecessarily wastes considerable resources as well as causing significant side-effects.
Dr. Thurtle and Dr. Gnanapragasam have since carried out a randomised study of almost 200 prostate cancer specialists in which they gave some clinicians access to the tool and a series of patient vignettes, while others received the vignettes only. In most cases, the clinician overestimated the risk of the patient dying from the cancer, compared to the estimate given by PREDICT, going on to recommended treatment in many cases and overestimate how successful this treatment would be. When given access to the tool, the clinicians were less likely to recommend treatment in good prognosis cancers.
Dr. Gnanapragasam says that the development of PREDICT Prostate has only been possible because of the intactness of records available through Public Health England—the tool was developed using data from over 10,000 UK men recorded in the East of England. This regional registry, he says, is one of the highest quality and most comprehensive data sets available both in the UK and internationally. The data was then validated externally in a sample of 2,500 prostate cancer patients in Singapore. The web tool was developed in collaboration with the Winton Centre for Risk and Evidence Communication
Source: Read Full Article